Typical UIP
There is peripheral reticulation and honeycombing involving all 5 lobes. The posterior lower lobes are more extensively involved.
CT study
Basic viewer tools:
 |
Scroll tool: When active, click and drag on the image to scroll through the series of images. |
 |
Adjust window/level: When active, click and drag on the image to adjust the brightness and contrast of the image, to bring out detail in different parts of the image. Common presets are available in the dropdown menu beside the button. |
 |
Pan tool: When active, click and drag the image to move the image within the viewport. |
 Open full study in Pacsbin viewer
Open full study in Pacsbin viewer
Probable UIP
There are peripheral areas of ground glass attenuation with superimposed reticulation and traction bronchiectasis. The posterior lower lung zones and the anterior upper lung zones are more involved. Honeycombing is not identified.
CT study
Basic viewer tools:
|
Scroll tool: When active, click and drag on the image to scroll through the series of images. |
|
Adjust window/level: When active, click and drag on the image to adjust the brightness and contrast of the image, to bring out detail in different parts of the image. Common presets are available in the dropdown menu beside the button. |
|
Pan tool: When active, click and drag the image to move the image within the viewport. |
Open full study in Pacsbin viewer
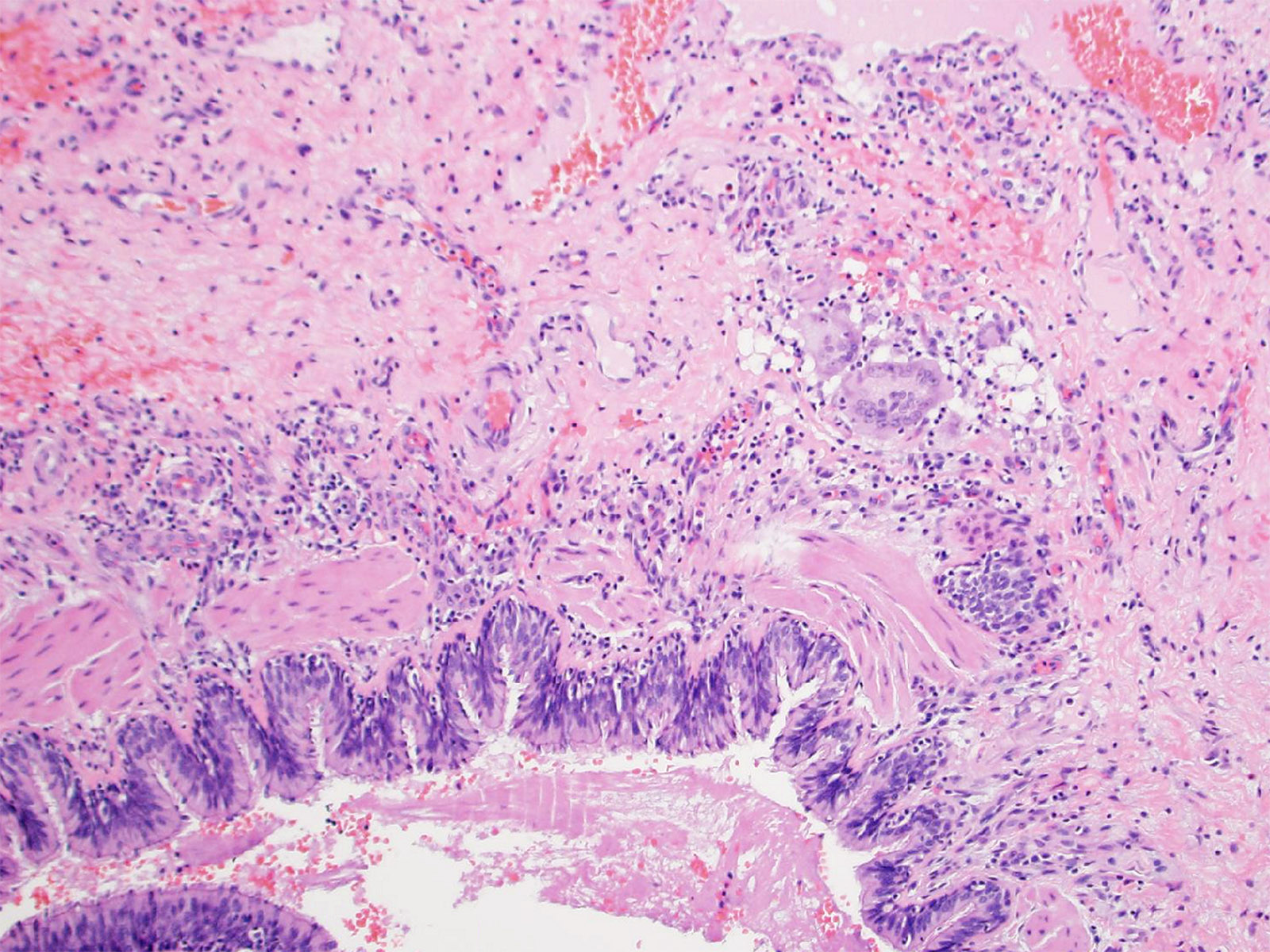
Histology
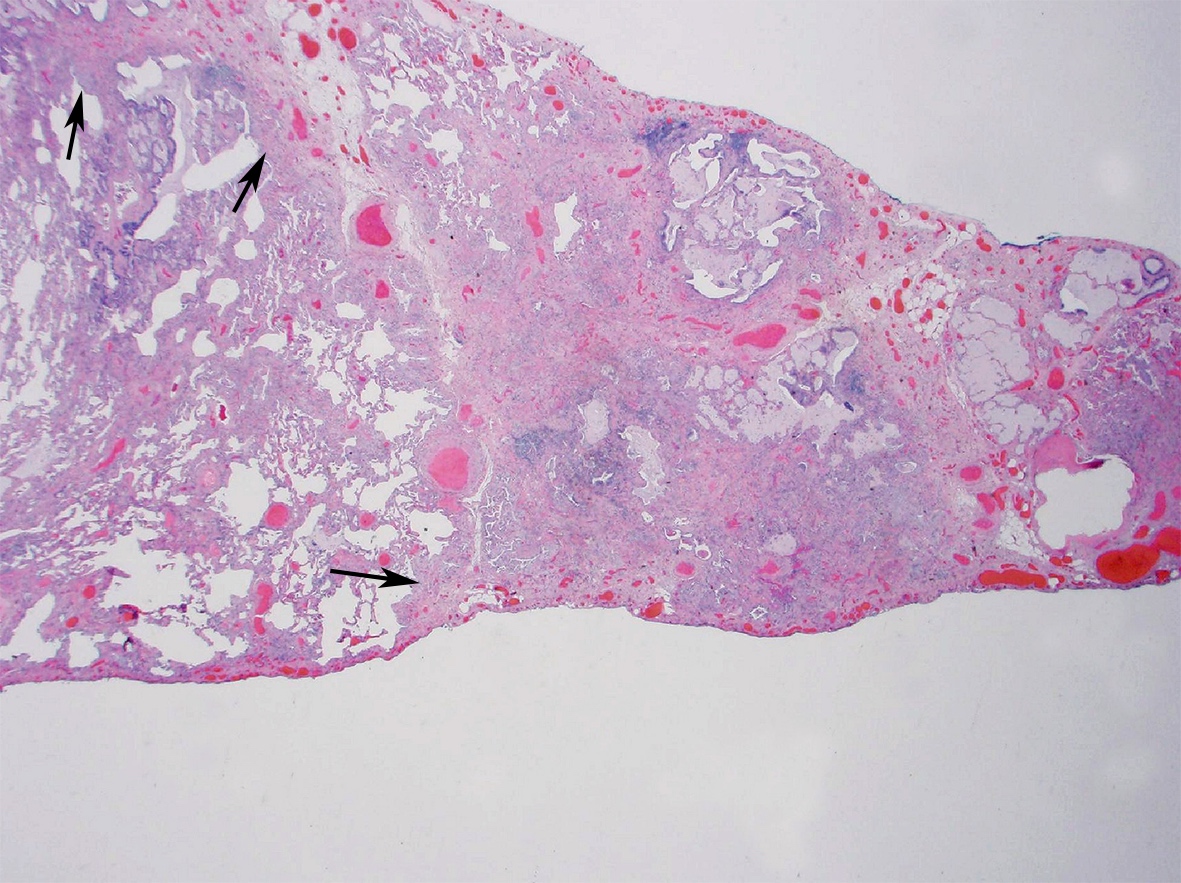
Low power magnification of lung demonstrates areas of end-stage fibrosis/honeycombing alongside lobules where there is patchy mainly paraseptal fibrosis with fibroblastic foci (arrows), indicating UIP on histology.
Indeterminate for UIP/IPF pattern
There are patchy areas of ground glass opacity with a faint reticular pattern and minimal traction bronchiectasis. The opacities are both peripheral and peribronchiolar in distribution. All 5 lobes are involved.
CT study
Basic viewer tools:
|
Scroll tool: When active, click and drag on the image to scroll through the series of images. |
|
Adjust window/level: When active, click and drag on the image to adjust the brightness and contrast of the image, to bring out detail in different parts of the image. Common presets are available in the dropdown menu beside the button. |
|
Pan tool: When active, click and drag the image to move the image within the viewport. |
Open full study in Pacsbin viewer
Histology
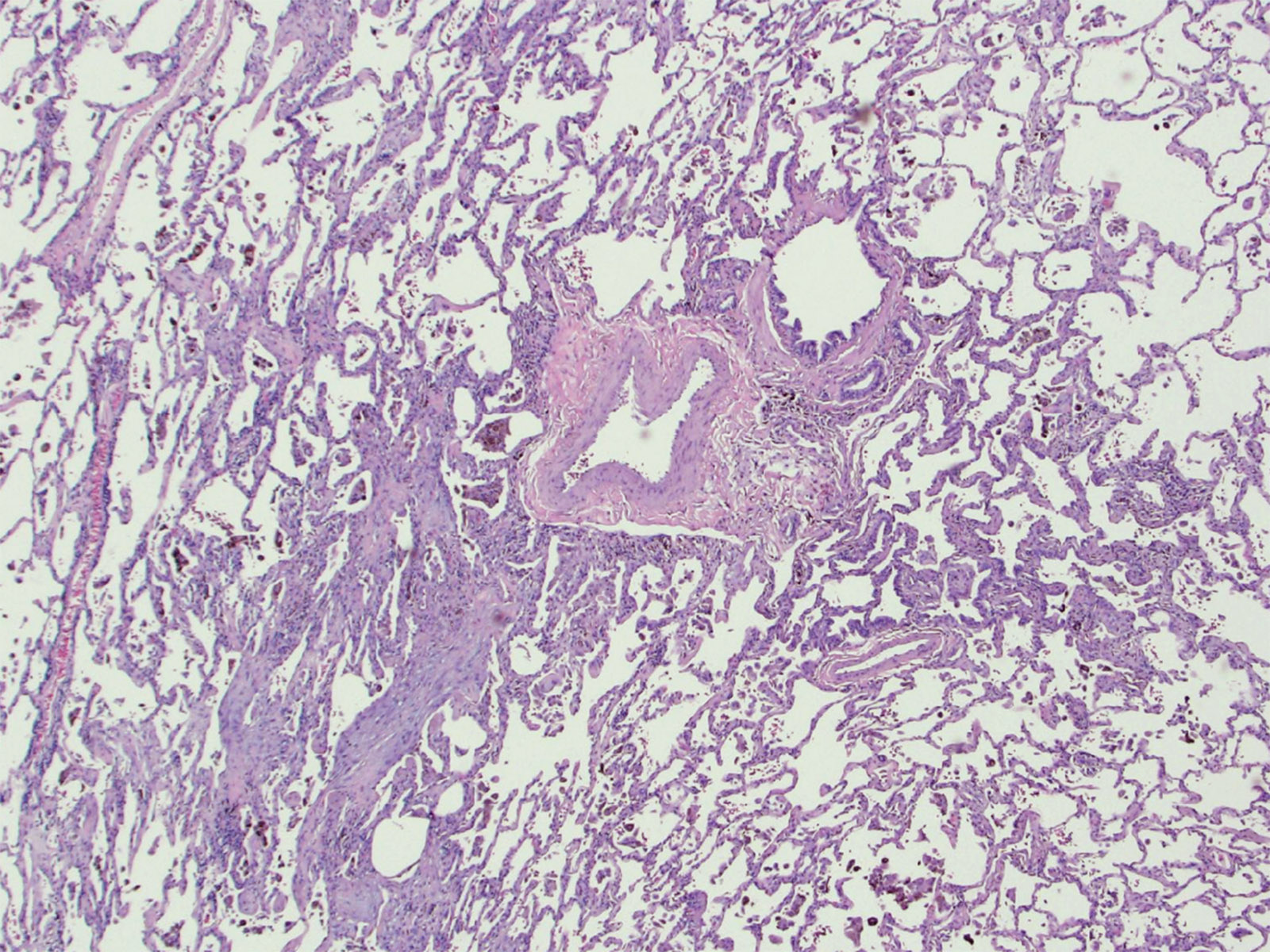
Intermediate power magnification of lung demonstrates smoking-related injury manifesting primarily as respiratory bronchiolitis (RB) characterized by accumulation of smoker’s pigmented macrophages in airspace surrounding bronchioles as well as mild peribronchiolar fibrosis and chronic inflammation. This is a "non-UIP" pattern and, whilst RB may be a separate smoking-related finding in patients with IPF, the patient was deemed not to have IPF on clinical-radiologic-pathologic consensus based on indeterminate CT findings, a history of smoking and features only of RB on biopsy.
CT features most consistent with non-IPF diagnosis
The CT shows subpleural reticular abnormality and honeycombing which is almost confined to the upper lung, associated with marked upper lung volume loss and architectural distortion. These findings are strongly suggestive of a non-IPF diagnosis.
CT study
Basic viewer tools:
|
Scroll tool: When active, click and drag on the image to scroll through the series of images. |
|
Adjust window/level: When active, click and drag on the image to adjust the brightness and contrast of the image, to bring out detail in different parts of the image. Common presets are available in the dropdown menu beside the button. |
|
Pan tool: When active, click and drag the image to move the image within the viewport. |
Open full study in Pacsbin viewer
Histology
Intermediate power magnification of lung demonstrates poorly formed collection of multinucleate giant cells and a few histiocytes in the adventitia of a bronchiole. Radiologic-pathologic consensus was chronic hypersensitivity pneumonitis.